Anti-Psychiatry
John Huddleston
"I know so many bad jokes. At least I didn’t invent them. Jimmy McKenzie was a bloody pest at the mental hospital because he went around shouting at his voices. We could only hear one end of the conversation, but the other end could be inferred in general terms at least from; ‘Away tae fuck, ye filthy bastards. . . ‘ It was decided at one and the same time to alleviate his distress and ours, by giving him the benefit of a leucotomy. An improvement in his condition was noted. After the operation he went around no longer shouting abuse at his voices but, ‘What’s that? Say that again! Speak up ye buggers, I cannae hear ye!’
R.D. Laing (1984:146)
INTRODUCTION
The term ‘anti-psychiatry’ was coined in the early 1960’s by Dr. David Cooper. The term has come to symbolise a loose confederation of psychiatrists, psychologists, psychiatric nurses, social and welfare workers, lay people and so-called patients who oppose and offer a critique of ‘traditional mental health practice and treatment’.
Cooper (1980) defines anti-psychiatry as:
"1. Reversing the rules of the psychiatric game; countering medical power as embodied in the diagnosis, the principal way of not leaving the other in the humiliation ceremonial of psychiatric interrogation (’interview’). . .
2. Abolition of hierarchical authority structure, recognising that the madman may express the central authority. . .
3. Attentive non-interference aimed at the opening up of experience rather than its closing down. This means the abolition of all forms of shock treatment (insulin and electric in all forms). . .
4. The ending of all forms of sexual repression between any two (or more) people who desire it."
This chapter will examine anti-psychiatry in terms of its historical and intellectual origin, the views of its major exponents and its implications for social welfare practice. In particular, the views of R.D. Laing, David Cooper and Thomas Szasz are outlined. Also some examples of alternatives to traditional methods of dealing with the so-called ‘mentally ill’ are considered.
Historical/Intellectual Origin
The anti-psychiatry movement has its origin in a number of diverse sources. The views of the ‘labelling’ theorists have influenced anti-psychiatrist viewing ‘mental illness’ as a form of deviance that is controlled through social/political tools and technologies present in society.
The work of Erving Goffman and others have also influenced the views of anti-psychiatrists in terms of power and the effects of organisational structures and ‘cultures’ upon the behaviour of inmates in psychiatric or institutional settings. Further, the work of Gregory Bateson and the ‘Palo Alto’ group have influenced the anti-psychiatrists in their contention that ‘mental illness’ is an appropriate, or at least understandable, reaction to disturbing social interactions. Finally, existentialism has provided the philosophical basis for anti-psychiatry explanations for unique, alternative, or disturbing individual experiences or behaviour.
George Herbert Mead (1934) raised a number of issues regarding the nature of social problems. Mead’s argument was that social problems arise out of interactions that come to be labelled ‘deviant’, and that social problems are in fact violations of social rules and expectations. His view of social problems was not unlike those expressed by Rubington and Weinberg (1981:186) where they define the labelling perspective in these terms:
"A social problems or social deviant is defined by social reactions to an alleged violation of rules and expectations. This perspective focuses on the conditions under which behaviours or situations come to be defines as problematic or deviant."
Writers like Peter Conrad (1975:12-21), while applying labelling theory to the notion of ‘disease’, pointed out that medical problems like hyperkinesis were ‘discovered’ by pharmaceutical companies and U.S. Government action, rather than in discovery by the medical profession in search of new diseases.
Contrasting labelling theory with the view that ‘mental illness’ exists, Scheff (1973:53) observed it was:
"A point of view which is an alternative to the medical model, and which acknowledges the culture bound nature of mental illness."
Scheff (1973:49) argues, using labelling theory, that mental illness is in fact residual rule breaking and that traditional medical diagnosis "reify and legitimate the prevailing order at the expense of other possible worlds". Scheff (1980:261-263) argued further that conceptual models of ‘mental illness’ are basically concerned with individual systems, rather than social ones. Scheff (1980:263) observed:
"The medical metaphor of mental illness suggests a deterministic process that occurs within the individual: the unfolding and development of the disease."
Scheff (1966:25) adopts the position that psychiatric symptoms are "labelled violations of social norms, and stable mental illnesses to be a social role".It is seen when discussing the anti-psychiatrists, the effect labelling theory has had on their perceptions and attitudes toward ‘mental illnesses.
The work of Erving Goffman and others has had a profound effect on anti-psychiatry and the ways anti-psychiatrists perceive mental hospitals and there effects on patients. Goffman, while working as an aide in a psychiatric hospital, saw the mental hospital with its hierarchy and politics designed to meet organisational (staff) needs, at the expense of the needs of the patients. The culture of the ward created an environment where individual identity, for the patients, was sacrificed in the interests of the smooth running of the institution. Goffman (1975:306) says:
"Whatever the patients social circumstances, whatever the particular character of his ‘disorder’, he can in this setting be someone whose problem can be approached, if not dealt with, by applying a single technical-psychiatric view."
Goffman also found that much of what was seen in the mental hospital as symptomatic behaviour was, in fact, a response to ward policy and rules, as opposed to a manifestation of a psychiatric disorder. The work of Perucci (1975) and others have gone on to affirm the Goffman argument that so-called ‘bizarre’ or symptomatic behaviour is a function of the hospital operation procedures, or ‘treatment’ modes used. These studies have had a significant effect on anti-psychiatry, particularly the views of Thomas Szasz.
The work of Gregory Bateson has had a profound effect on anti-psychiatry. Bateson’s theory of the ‘double bind’ influenced the ways in which R.D. Laing and David Cooper considered so-called ‘schizophrenic’ interactions and their analysis of families from which these ‘mentally ill’ come from.
They both have accepted the conclusion of Bateson that ‘schizophrenia’ has its origin in people’s reactions to double-bind situations. The double-bind situation being described by Bateson (1973:178-179) as being interactions characterized by:
"1. Two or more persons.
2. Repeated experience.
3. A primary negative injunction.
4. A secondary injunction conflicting with the first at a more abstract level, and not unlike the first enforced by punishment or signals which threaten survival.
5. A tertiary negative injunction prohibiting the victim from escaping the field."
The double-bind’ is seen by Laing and Cooper as a situation where the person, who is the victim of it, has no means of responding to it in a meaningful or rational way and for whom escape is impossible. The double-bind is a no win situation where you are damned if you do and damned if you don’t. Those who are labelled a schizophrenic are typically those who use ‘schizophrenic behaviour’ as a means of survival. The book Catch 22 by Joseph Heller is a satirical or black comedy way of illustrating this phenomenon.
Finally, existentialism is the major philosophical force behind most of anti-psychiatric thinking. The anti-psychiatrists tend to reject traditional scientism and the deterministic thinking behind it, while accepting the notion of the existential ‘phenomenology of experience. The work of both Laing and Cooper reflect the ideas of existentialists such as Sartre, Heidegger and others. They all stressed the uniqueness of individual experience, the subjective nature of ‘reality’ and a rejection of the medical model concept of ‘mental illness.
The Anti-Psychiatrists
The major contributors to anti-psychiatry are R.D. Laing, David Cooper and Thomas Szasz. Peter Breggin is also mentioned as he is a current practicing psychiatry who holds similar views to the others mentioned here.
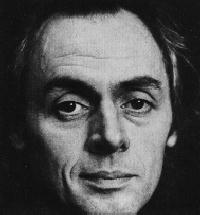
The most well know exponent of anti-psychiatry during the last 1960’s and 70’s has been the late R.D. Laing. Ronald David Laing, (pronounced ‘Layng’), psychiatrist, poet, mystic, philosopher, guru was born in Glasgow, Scotland on October 7, 1927 at 17.15. That this timing was significant to Laing was later mentioned by him in The Facts of Life (1977:76) where he wrote:
"At 17.15 almost every day for several years, I feel like a drink of vodka. Sometimes I restrain myself. Sometimes I let myself have it. Why do I want it then? I often know when it is 17.15 by that feeling that comes over me. Why? Has it anything to do with the hour of my birth 17.15? Or with my idea of the hour of my birth?
 Laing’s parents, David and Amelia, were lower middle class Presbyterians. His mother’s family considered themselves to be Celtic Protestants from the south west of Scotland. Laing’s father spent much of his working life as an electrical engineer with the Corporation of Glasgow. Laing’s father’s side claimed a family relationship to Robert Louis Stevenson.
Laing’s parents, David and Amelia, were lower middle class Presbyterians. His mother’s family considered themselves to be Celtic Protestants from the south west of Scotland. Laing’s father spent much of his working life as an electrical engineer with the Corporation of Glasgow. Laing’s father’s side claimed a family relationship to Robert Louis Stevenson.
During many of his early years, Laing spent much of his time playing alone. At an early age he learned to be sceptical about what others taught him. Laing (1986:40-41) recalls how at the age of five he was informed by his parents that they had played Santa Claus and that . . . "this incident made me wary of believing anything because I was told it. Later he decided". . . at the age of 13, for instance, that I would make a point of forgetting anything that was painful", (Sedgwick 1982:71). In his teen years he became interested in existential philosophy and read extensively the works of Martin Heidegger, Ludwig Binswanger and particularly Jean-Paul Sartre. Laing later reflected that as a young man he craved "the fame of a wise man", (Mezan 1976-lix-lxii), and vowed he would have a published book by the age of thirty, (he did).
He graduated from Glasgow University in 1951. Initially Laing was interested in neurosurgery. After his graduation from medical school he worked at the Glasgow and Western Neurosurgical Unit situated at Killearn for six months.
Laing was called up into the British Army where he remained between 1951-1953. Much of his work in the British Army was at the British Army Psychiatric Unit at Netley where he worked on an ‘insulin ward’. Psychiatric patients were place in deep comas and given insulin at a level where they would have epileptic seizures. As well, this unit used electro-convulsive therapy. As with insulin treatment, this therapy was used to deal with depression and other ‘worrying’ symptoms seen in the soldiers. Laing remained with this unit for over a year.
After leaving Netley Laing was frequently involved in assessing soldiers whether they were in fact ‘mentally ill’, or simply faking their symptoms, (malingering).
It was during this period Laing began to seriously question his work. Laing (1986:98) stated:
"I was just beginning to suspect that insulin and electric shocks did more harm that good. I had begun to have to call into question my own sanity, because I was beginning to suspect that insulin and electric shocks, not to mention lobotomy and the whole environment of the psychiatric unit, were ways of destroying people and driving them crazy if they were not so before and crazier than they were".
After a year at Netley Laing was transferred to Northern Command at Catterick in Yorkshire in charge of a clinical and detention ward of Catterick Military Hospital, finally being discharged from the Army with the rank of Captain in 1953 at the age of 26.
After his discharge from the Army Laing went to work at Glasgow’s Gartnavel Royal Hospital. In 1957 he joined the Tavistock Clinic in London.
It was from much of his early work in Glasgow that Laing obtained the case studies for his first books, that began with The Divided Self in 1957. It was at this time that Laing clearly began to question the traditional notions about ‘schizophrenia’ as a disease. This was in part because, unlike his colleagues, Laing could not perceive symptomatology the way they appeared to be able to. Early in his work in Glasgow, Laing spent much of his time, along with the nursing staff, drawing sociograms of the ward patients and staff. He discovered during this time that ‘disturbed’ patient behaviour was often a function of ward relationships and interactions and made perfect sense when viewed within that context. What often appeared to be bizarre, inexplicable behaviour became revealed as meaningful, understandable activity. Within the apparent chaos of the ward there was meaning. The Divided Self is Laing’s view of ‘schizophrenia’ based on these observations.
Laing (1978:45, (1981:94) acknowledges the influence that Gregory Bateson and the ‘Palo Alto Group’ have had on his won thinking. His book Self and Others (1961 revised 1969) focused on the interactive aspects of ‘schizophrenia’, rather than the individual’s experience that Laing had focused on the Divided Self. This focus was developed further as Laing (1970) explored how people with the family setting can organise and conspire against another member of the group. Laing (1970:90) saw this as a collusion that was:
". . .a ‘game’ played by two or more people whereby they deceive themselves. . . an essential feature of this game is not admitting that it is a game".
Laing’s third book was one co-written with his friend Aaron Esterson, (who graduated from medical school the same year as Laing) and was called Sanity, Madness and the Family. Unlike his previous works, this book focused on the family, rather than individuals caught up in the psychiatric ward situation.
During the early 1960’s Laing continued developing his existential views. In 1964 he had written Reason and Violence: A Decade of Sartre’s Philosophy with David Cooper. This book, vintage watered down Sartre, offered some clear insights into Sartre's phenomenology, (particularly the chapters written by Cooper). Like Sartre, Laing began more and more to focus on the nature and characteristics of ‘experience’ of the so-called ‘mentally ill’, rather than considering ‘schizophrenia’ as a disease entity.
Through these years and later, Laing questioned more and more the notion of what constituted ‘normality’. Laing (1981:23-24) states:
What we call ‘normal’ is a product of repression, denial, splitting, projection, introjection, and other forms of destructive action or experience. It is radically estranged from the structure of being. . . normal men have killed perhaps 100,000,000 of their fellow normal men in the last fifty years."
Who is sane and who is crazy? The man who thinks he can blow up the world or the man who actually can? (C.f. Brown 1973:64).
Certainly Laing has come to oppose the diagnostic process and categories of traditional psychiatry. Laing (1972:14) attacks the traditional medical model position by saying that:
"If you are ill from our point of view and you do not think you are ill from your point of view, that this is further token of how ill you are"
Laing (1982:43) goes on to point out that traditional ‘objective’ assessments of human behaviour regard
". . . some experience as worthless and destructive, per se, that we feel that the biological process which accompanies them must be pathological".
For Laing the so-called psychotic is the name we use for the other person in a disjunctive relationship of a particular kind, (Gordon 1972:53). This disjunctive relationship is amplified by traditional therapy, which comprises a highly selective series of destructive interactions. Laing (1981:102) stated that:
"What we see sometimes in some people whom we label and ‘treat’ as schizophrenics are the behavioural expressions of experiential drama. But we see this drama in a distorted way that our therapeutic efforts tend to distort further. The outcome of this unfortunate dialectic is a forme frustre of a potentially natural process, that we do not allow to happen".
‘Schizophrenia’ is, from Laing’s perspective a natural process. He sees it as a strategy that people use for identity and survival.
Stiegler (1972:101) stated that Laing sees ‘schizophrenia’ as a label people apply to others in some circumstances and is not a disease entity like pneumonia, but is a social fact and a political event.
Laing (1979:39) doesn’t like using psychiatric terms and regarding ‘schizophrenia’ says:
"I’m unhappy about using the term schizophrenia at all. But it would be somewhat whimsical to eliminate it from my vocabulary since it is on the lips of so many".
True to labelling theorists, Laing (1978:38 & 52) views ‘mental illness’ labels as reflecting societal attitudes and functioning as a ‘straight jacket’. Since Laing sees ‘schizophrenia’ as a natural process the ‘schizophrenic episode’ is a natural ". . . resource a human being calls upon when all else seems impossible", (Laing 1972:11).
Further, Laing (1972:13) sees ‘schizophrenic experience’ as resulting from, and meaningful when, social situation are explored and understood. Of particular interest are the interactions that develop from the family situation. Laing considers the social interactions of the family to be intrusive, stifling and confusing in terms of personality development and self-identity. The family is seen as a controlling set of interactions where the so-called ‘schizophrenic’ finds himself/herself the victim of ‘collusive pairing’ and double-binds that make the world an impossible place. Laing (1976:89) says of the family:
"So we are a happy family and we have no
Secrets from one another
IF we are unhappy/we have to keep it
secret/
and if we are unhappy that we have to
keep it a secret
and unhappy that we have to keep
secret/the fact/that we
HAVE to keep it a secret
and that we ARE keeping all that
Secret.
But since we are a happy family you can
see this difficulty does not arise".
Laing (1971:14-16) cites the example of ‘Jane’ who at the age of 17 presented as ‘early schizophrenia simplex" and was absorbed in a continuous game of tennis. She appeared to assume the identity of all the elements of tennis including the crowd, the players, the court and especially the ball. Viewed in isolation her behaviour seems bizarre, but she was trapped within a series of family games. In these games she was the tennis ball hit back and forth between her parents. Mother would turn to Jane and say ‘Tell your father to pass the salt’. Father would turn to Jane and say ‘Tell her to get it herself’. Laing reports that after three months she saw the connections between tennis and her family. Two years later she left the family and ‘has been active in the world for ten years’.
If traditional psychiatry and treatment are destructive and ‘psychotic episodes’ are natural, then what form of treatment should be used? Kingsley Hall provides an example of Laing’s anti-psychiatry in practice.
Kingsley Hall as built about 80 years ago by two wealthy unmarried sisters in London who fancied themselves as being social workers. After their deaths the three story building was administered by a trust. It was said that in 1931 Gandhi stayed there while visiting London.
Laing and the Philadelphia Association, of which he was the chairman, occupied the premises from 1 June 1965 - 31 August, 1970. The core group consisted of Laing, David Cooper, Aaron Esterson, Sid Briskin, (a social worker), Leon Redler, Joe Berke, Morton Schatzman and Jerome Liss. During the work of Kingsley Hall therapists were to come and go with Laing remaining throughout its entire existence. A total of 113 patients stayed at Kingsley Hall.
At Kingsley Hall there was no structured ‘therapy’. No drugs other forms of thought control were applied, with ‘patients’ allowed to experience the full force of their ‘episodes’. The ‘therapists’ lived with the ‘patients’ in Kingsley Hall and everyone addressed each other by their first names. Policy decisions were group decisions. This form of ‘therapy’ was a distinct destructuring of the therapeutic environment and within this context ‘patients’ typically manifested various forms of regression. Laing (1978:46) describing the process of regression as "perhaps the most taboo movement of all".
Laing further observed that while much has been written on the subject of regression, that it is a phenomenon that is little understood.
Kingsley Hall’s most famous ‘patient’, Mary Barnes, serves as a good example to illustrate the anti-psychiatry of Laing. When she first arrived at Kingsley Hall, Mary was 45 years old. She had worker in hospitals as a nurse and had been diagnosed as ‘chronic schizophrenic’ after repeated admission into psychiatric hospitals. Her account of her experiences at Kingsley can be read in a book she co-wrote with Joe Berke, Mary Barnes: Two Accounts of A Journey Through Madness.
Her regression at Kingsley Hall is vividly describe in Barnes (1973:174) where she says:
"Flection: The act of bending or the state of being bent. That’s how I was at Kingsley Hall, bent back into the womb of rebirth. From this cocoon I emerged, changed to the self I had almost lost. The Buried me, entangled in guilt and choked with anger as a plant matted in weed, grew anew, freed from the knots of my past".
Kingsley Hall provided the environment for her ‘journey in the womb’. In Kingsley Hall the environment had been opened up to experience, rather than creating a shut down world. As was previously mentioned, the ‘therapists’ and ‘patients’ both lived there and contact was on a 24 hour basis. Kingsley Hall was the definitive anti-psychiatry practice. Kingsley Hall and Laing’s approach to ‘treatment’ was summarised by Laing (1972:15) as follows:
"We try to follow and assist the movement of what is called ‘an acute psychotic episode’ instead of arresting it".
Toward the end of the 1960’s Laing began to discuss more the political aspects of his work and to view things globally. In The Politics of experience and the Bird of Paradise, Laing discussed more openly the political nature of the arm’s race and the potential for massive global destruction. In July 1967 Laing participated in ‘The Congress on the Dialectics of Liberation’. At this conference he presented his paper ‘The Obvious’ where he drew global parallel between his observations on the psychiatric ward and the behaviour of nations on a universal scale.
In the end, Laing sees traditional ways of relating and interacting as an exploitation of other people’s experience. ‘Experience’ within Western society is subject to ‘mystification’, which Laing defines as ‘an apparently reasonable misrepresentation of what is actually the case’. He sees ‘mystification’ as an attempt to create a false consciousness within society and within ourselves. The ‘mystification of experience’ is a political tool used to exploit, control and manipulate others. Laing (19884:49) states:
In order to rationalise our industrial-military complex, we have to destroy our capacity to see clearly any more what is in front of, and imagine what is beyond, our noses. Long before a thermonuclear war can come about, we lay waste our own sanity. We begin with the children. It is imperative to catch them in time. Without the most thorough and rapid brain-washing their dirty minds would see through our dirty tricks. Children are not yet fools, but we shall turn them into imbeciles like ourselves, with high I.Q.’s if possible".
Laing died on the south coast of France on August 23, 1989.
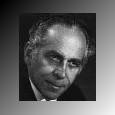
David Cooper, a former colleague of Laing, is another of the dominant personalities with the anti-psychiatry movement. Cooper was born in Cape Town, South Africa in 1931 and obtained his medical degree in 1955. In the early 1960’s it was Cooper who coined the phrase ‘anti-psychiatry’ and in 1962 set up Villa 21 as an ‘anti-psychiatry’ ward in Shenley Hospital.
The purpose of the ward, (like Kingsley Hall that followed it), was to destructure the ward environment. ‘Patients’ and ‘staff’ wore no uniforms and sought to deal with ‘emotional’ problems through non-responsive involvement. Cooper (1972:43) said of his therapeutic approach that it
". . . resides centrally in the native praxis of not depriving, based on the realisation that in this context of relationship no one can deprive any one of anything".
Cooper (1967:29-30) sees ‘mental illness’ in terms of society labelling non-conformists ‘bad’. Cooper (1974:29) argues that mental health is based on notions of conforming to arbitrary social norms so vague that they "deprive themselves of operational significance". He, like Laing, sees the origin of ‘mental illness’ as resulting from bizarre interactions, often within the context of the family.
Cooper argues that through complex ‘double-binds’, the family regulates not only permissible behaviour, but also permissible experience. Cooper view the fundamental role of the family being to politically control its members.
Cooper (1974:84) asserts that the middle class family is itself a ‘double-bind’ institution when he says:
"The conventional bourgeois parental couple is both the super ambisexual pig and a massive bacon factory. This is its central ambiguity. Those who escape through some fire exit or in the disguise of a workman, tend to end in a great porcine bin or in a prison or in other abattoirs. A few, through great travail and pain, manage to escape and become sane. . ."
Cooper (1980:41-51) also views ‘madness’ as an attempted restructuring process that, if left alone, can result in a "renewal of oneself".
Cooper perceives traditional psychiatric institutions as symbolising political repression against the working class and as a tool used to suppress political discontent. Cooper, along with Laing, was involved in Kingsley Hall, but split from him well over a decade ago.
Cooper has characterized Laing as becoming more conservative and conformist as he got older and having ‘sold out’ to the trappings of fame.
Recent years have found Cooper globe trotting, particularly in South America, where he has encouraged the development of ‘anti-psychiatry’ units in third world countries.
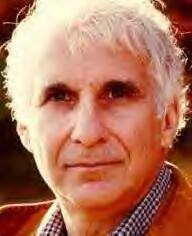
Finally, much of anti-psychiatry’s critique of traditional psychiatry is to be found in the work of Thomas Szasz. Szasz uses labelling theory to assert the fallacy of arguing that behavioural issues can be seen within the same framework of physical diseases. Szasz has consistently contended that there is no such entity as ‘mental illness’. What does exist has been the medicalisation of behaviour, in that deviant behaviour has come to be defined as ‘sick’, as opposed to being ‘bad’. The result of the medicalisation of deviance has been those who have deviated from supposed social norms have been compartmentalised, devalued, treated as patients and deprived of their civil liberties.
 Dr. Szasz is a civil libertarian who adopts the view that the medical industry has constructed the ‘myth of mental illness’. Szasz (1964:21-28) argues that psychiatric diagnosis does not describe the persons ‘state of mind’, but is a process that demeans and degrades the victims of this diagnostic process. Szasz (1973a:209) asserts that mental health classifications are used to "legitimate social control" by powerful professional groups upon those labelled as problematic. Behaviour, according to Szasz, cannot be divorced from the social context in which it happens. Szasz (1973b:11) points out that the concept of illness, whether bodily or mental, implies a deviation from some clearly defined norms. In the case of ‘mental illness’ these norms are clearly developed within cultural and social situations.
Dr. Szasz is a civil libertarian who adopts the view that the medical industry has constructed the ‘myth of mental illness’. Szasz (1964:21-28) argues that psychiatric diagnosis does not describe the persons ‘state of mind’, but is a process that demeans and degrades the victims of this diagnostic process. Szasz (1973a:209) asserts that mental health classifications are used to "legitimate social control" by powerful professional groups upon those labelled as problematic. Behaviour, according to Szasz, cannot be divorced from the social context in which it happens. Szasz (1973b:11) points out that the concept of illness, whether bodily or mental, implies a deviation from some clearly defined norms. In the case of ‘mental illness’ these norms are clearly developed within cultural and social situations.
Szasz sees those defined as ‘crazy’ as suffering from ‘problems in living’. Their problem often has as its nexus the fact that they do not live up to the expectations of others. Szasz sees so-called ‘psychotic episodes’ as often the result of game playing where the victim sees to use various game strategies in order to survive social oppression, (Sedgwick 1982:149-151).
Szasz’s solution, different from the other anti-psychiatrists, is the abolition of all involuntary hospital admissions and the allowance of private practice therapists to provide a service to those who freely chose to avail themselves of it.
It is Szasz contention that it is in the role of ‘patient’ that those who deviate from social norms are typically denied natural justice and held unaccountable for their behaviour. Often, the legal system uses the notion of ‘mental illness’ to lock up people against their will for prolonged periods of time without the people concerned having their day in court. These violations of human dignity extend even further to people being involuntarily incarcerated indefinitely even though they have engaged in no illegal behaviour. The violation of the human rights of the so-called mentally ill in Western countries by the medico-legal establishment is no less insidious than the mental atrocities perpetrated on political dissidents in the former Eastern Bloc of nations.
Szasz argues that justice is denied in other ways as well. John Hinckley Jr., the attempted assassin of President Reagan, never stood trial at all, as it was contended he was unfit to plead due to ‘mental illness’. Patty Hearst, former member of the Symbionese Liberation Front and well know rich girl, avoided spending decades of her life in prison, when she argued she was not fully responsible for her illegal behaviour. She claimed that she had been ‘brainwashed’ after she had been kidnapped in Berkeley, California. Szasz notes that this sudden flash of insight concerning her indoctrination happened after she met with expensive psychiatrists and slick lawyers hired by her multimillionaire parents.
In both of the above instances Szasz feels that justice was denied, based on the myth of diminished responsibility caused by the ‘mental state’ of the defendants. Szasz would argue that the plea of ‘mental illness’ or ‘diminished responsibility’ should have not role in the context of the legal system and that it is merely a fraud used to increase the power of the medical industry.
Recent events in Australia have shown a ‘psychiatric’ path in the legal system similar to that of the United States. The media flooded the Australian public with so-called experts who pontificated on the state of mind of Strathfield murderer Wade Frankum. These arrogant psycho-quacks offered a potpourri of explanations fro his behaviour ranging from him family background, association with prostitutes and exposure to pornography. Some of these psycho-babble entrepreneurs only assessed his psychological state during the rampage, but argued that society collectively was to blame for his behaviour. The analyses of the clairvoyants of the psychosexual arena were all the more bizarre in that none of them had actually met Frankum.
Another recent case that illustrates Szasz’s points regarding psychiatry and its involvement in the criminal justice system was the case of serial killer John Wayne Glover who, it was argued by some psychiatrists, was mentally ill and not responsible for his actions. Glover himself, sought to get some mileage out of the psychiatric game when he addressed his jury offering a tear ridden speech regarding the unfortunate events of his background. In his speech he cleverly implied that he, rather than the tragic women he murdered and their loved ones, was the victim. Fortunately, the hogwash he presented before the jury had no impact on his sentence and he will hopefully spend his remaining days behind prison walls.
Like their American counterparts the cases of Frankum and Glover illustrate the points Szasz make regarding the medicalisation of the legal system by psychiatry. It perhaps suits relatives of these murders to perceive them as sick, while Szasz sees them as like John Hinkley Junior as being merely bums.
Szasz denies that he belongs in the ‘anti-psychiatry’ camp and would probably express hostility that his chapter has placed him with David Cooper and R.D. Laing. Szasz is not at all shy about expressing his dislike for both of them. Szasz (1984:45) describes Laing and Cooper in the following terms:
"Cooper, the violate ‘madman’ the vulnerable, frightened child. The fooler and the fooled. What a perfect pantomime of madness and mad-doctoring! Cooper has a big heart that bleeds for his victims, especially of his own imaginings. His compassion has become cancerous and has all but destroyed him. Laing, on the other hand, has a good nose for business - in particular, for selling his dramatised impersonations of himself. . . Cooper is often wrong-headed, but he is honest, Laing is often level-headed, but is he ever honest?"
It is not fair to tar Dr. Peter Breggin with the label of Anti-psychiatry, yet he bears some common characteristics to Cooper, Laing and Szasz, yet is more contemporary. Peter Breggin was born in 1936 in Brooklyn N.Y. into an upper middle class family. He obtained a B.A. from Harvard in 1958 and M.D. from the Case Western University in 1962.
 Like the other, Dr. Breggin challenges contemporary conceptions of mental illness. He has been a critic of the use of SSRI’s to deal with issues like depression. Very much like Laing and Cooper he sees typical mental distress as a function of problems of living rather than merely medical problems to be solved by new technology and drugs. He has come out very much in opposition to various forms of drug use to treat behaviour ranging from the use of Ritalin through to Prozac. He has also opposed treatment strategies that have included ECT and psychosurgery. Like Szasz he views modern psychiatry as a political act with social control aspects. Like Szasz he equates some of the practices of psychiatry with those of a totalitarian state. He observes:
Like the other, Dr. Breggin challenges contemporary conceptions of mental illness. He has been a critic of the use of SSRI’s to deal with issues like depression. Very much like Laing and Cooper he sees typical mental distress as a function of problems of living rather than merely medical problems to be solved by new technology and drugs. He has come out very much in opposition to various forms of drug use to treat behaviour ranging from the use of Ritalin through to Prozac. He has also opposed treatment strategies that have included ECT and psychosurgery. Like Szasz he views modern psychiatry as a political act with social control aspects. Like Szasz he equates some of the practices of psychiatry with those of a totalitarian state. He observes:
The destructive impact of psychiatry upon our civilization has been given too little attention and the role of psychiatry in Nazi Germany almost no attention. It is entirely possible that without psychiatry the holocaust could never have taken "place.
He runs the Centre for the Study of Psychiatry which is a non-profit organisation devoted to looking at the role of psychiatry in the denial of human rights, squashing civil liberties and undermining the well being of the individual.
He is one of the few articulate voices challenging the medicalisation of experience and the social control aspects of the psychiatry industry generally and the drug business particularly.
This brief summary of anti-psychiatry has outline the basic principles of the approach. All those who fall into the anti-psychiatry camp share a common rejection of the 'medical model' of mental illness, as well as being in conflict with state run 'mental health' treatment programs. All show sympathy for the labelling approach to social problems and deviant behaviour.
It is important to stop here and acknowledge some alternative institutions that operate along anti-psychiatry principles, e.g. the work of Franco Basaglia within the psychiatric setting in Italy, former government policy in the Peoples' Republic of China and the work in 'New Haven' in the United States.
Franco Basaglia's work began in Gorizia, Northern Italy and much of his work considered here took place between 19962-19967. During the period he was involved within the Gorizian bureaucracy, Basaglia attempted to come to terms with abandoning established views of psychiatric assessment, treatment and incarceration. Basaglia was aware that psychiatric treatment and diagnosis were only parts of the problems of those labelled 'mentally ill'.
Basaglia (1980:185) reported that;
"It was necessary to look beyond the asylum at the role of psychiatry had in society at large: for the psychiatric diagnosis were rooted in the prevailing moral order, which defined normality and abnormality in its own rigid terms, and it was the class system itself which gave rise to the first of the 'lower orders' who made up the bulk of the psychiatric cases".
Basaglia and co-workers, using a Marxist framework, saw much of the problem of those labelled 'mentally ill' as being a function of power relationships reinforced within the institutional setting. In Gorizia he began the task of creating an environment where patients were more powerful. He became involved in changing ward structure and symbols of oppression within the total institution that constituted the psychiatric hospital. While these changes were enacted in Gorizia, Basaglia and his co-workers realised that merely changing the ward system was not enough and that a wider perspective was required.
In 1971 Basaglia set up work in Trieste.. There he began the same process of restructuring he had begun in Gorizia. This process involved, among other things, the unlocking of nine formerly locked wards, the removal of the use of uniforms by staff, abolition of compulsory treatment, including drug therapy and replacing therapy sessions with general meetings. At these general meeting staff and patients me to discuss and formulate ward policy. The use of psychiatric labels was eliminated and the purpose of all meeting in the hospital was for the purpose of 'consciousness raising'.
Community health centres were set up in Trieste, but were not functioning merely along former conventional public health lines. They were designed to be true support services for the powerless who constituted the patients, Basaglia (1980:192) reflected that:
"Although in many ways the project in Trieste might seem to resemble community health schemes elsewhere, it is important to distinguish it from psychiatric services which merely reproduce the old contradiction between therapy and the maintenance of public order".
Basaglia and his co-workers saw as their ultimate goal the abolition of the psychiatric hospital and the reintegration of its patients back into society. In 1970 Basaglia and his co-workers formed a national organisation called Psichiatria Democratica that conducted a number of campaigns in Italy to change the treatment of so-called 'mentally ill' citizens. They campaigned particularly in Northern Italy where they won funding to support non-institutionalized community dwellings, (see de Zulueta 1979). The Psichiatria Democratica sought to establish alliances with the trade union movement, as well as the Communist Party and other political factions. That Basaglia was fighting a national war became apparent when in 1972-3 strikes by the nurses union, controlled by the Christian-Democrats, against his policy changes in Trieste almost resulted in the halting of those changes.
At present Basaglia's work remains the largest scale on which anti-psychiatry principles have been implemented in the West within both institutional and social settings.
In the East in the Peoples Republic of China there have been large scale alterations to former practices in dealing with social deviance and rule breaking. While Russia and the Eastern nations by and large follow a Western style 'medical model' view of mental illness, (see Lader 1977 for a detailed discussion), the same cannot be said for China.
Illich (1977) equated closely the policies of the Chinese Government with those of anti-psychiatry when he state:
". . .seems close to an official doctrine in modern China, where mental illness is perceived as a political problem".
The view that deviance is a political act has led both China and Vietnam to establish reeducation camps after their successful revolutions, and may explain in part why Vietnam has virtually no psychiatric services in existence.
Often within the social systems of China and Vietnam some crimes such as theft and 'laziness' are seen as best handled in the workplace where reeducation takes place. In more extreme instances people are isolated from public gaze in reeducation camps.
It is difficult to assert that anti-psychiatry practices are used, or if the camps merely function along the lines of 19th Century mental asylums in the United States and Great Britain where the inmates were given 'moral therapy' to reintegrate them back into their respective communities.
Over the years a number of alternative structures and institutions have been set up around the world. 'New Haven' in the United States is an example of non-medical model assistance. The New Haven Halfway House was set up in 1967. It was established as a community for discharged mental patients, as well as students. Except for behaviour pertaining specifically to 'the community' people were free to regulate their own behaviour. However there were a number of rules that were seen as necessary for the survival of the project. In order to be admitted to the community the approval of all the residents was required. All residents were required to either have a job or be full time students. Residents were required to pay rent, keep their rooms clean, avoid physical violence and not have friends stay over for long periods. Also, residents were expected to attend resident meetings and participate in the decision making of the community.
In New Haven there was no treatment per se and the atmosphere was seen as one where people were able to experience the world in their own ways without therapy or drugs and work through their 'problems of living' without any therapy approach being imposed on them. A more detained discussion of this agency can be found in Jaffe (1972).
It is not possible in this short space to list all the organisations that may operate along anti-psychiatry lines. A number of alternative institutions such as various radical feminist lesbian separatist groups simply defy straight forward categorisation of the approach(s) they are using. Further, other agency operations were established during Laing's and Cooper's involvement with Kingsley Hall, which included the organisation of non-institutional 'households' in the London area. Other groups that have been involved in anti-psychiatry like activity in the U.K. have included the Mental Patients' Union of Britain. In Germany there has been the Sozialistisches Patientenkollectiv and the Groupes Information Asiles in France.
In the United States there have been alternative groups like the Radical Therapist Collective, the Mental Patients' Liberation Front and the Network Against Psychiatric Assault. Other groups like Synnanon and Scientology have frequently argued that they provide alternative conceptions to traditional psychiatric thinking, but it has been argued their operations do not frequently live up to their assertions. In the two previous organisations it is difficult to separate fact from fiction in light of extremely brutal attacks on them by the medico-political establishment.
Most recently the Church of Scientology has been at the forefront of attacks on the medical model of mental illness specifically and the psychiatric industry generally. The Citizens Commission on Human Rights (CCHR) was co-founded in 1969 by the Church of Scientology and Dr. Thomas Szasz, Professor of Psychiatry Emeritus at the State University of New York Upstate Medical University in Syracuse, to investigate and expose psychiatric violations of human rights. For example they describe various psychiatric disorders such as ADHD (Attention Deficit Hyperactivity Disorder as, "Psychiatry’s cash cow diagnosis". This applies to all of the recent invented disorders ranging from post traumatic stress disorder, post natal depression through to more traditional concepts such as schizophrenia.
Scientology argues, not unlike Dr. Breggin, that the intention of new disorders has evolved out of the desire for large drug companies to make ever increasing dollars out of both the private and governmental purses of the West. In terms of the use of shock therapy, Scientologists observe that:
"Ask the foremost psychiatrists and they have no explanation to justify why or how their ECT "works." It is literally as scientific as sticking one’s head in a light socket. Do it often enough and you will become disoriented, confused, lose your memory or even die."
The scientologists have enlisted the support of celebrities to carry their message. This has involved celebrities such as John Travolta, Lis Marie Presley and most notably Tom Cruise. They have used comments by notables such as the Fleetwood Mac Singer Stevie Nicks who notes:
"I went to a psychiatrist. It was a bad decision….[he] put me on this medication that nearly destroyed my career, nearly destroyed me, nearly destroyed my parents—because they just lost me for those years…."
It’s hard to know what the future will bring. The incessant litany of psycho-babble continues to intrude into daily existence. The social control institutions have become more invasive and powerful. Modern technology continues to increase the degree to which governments can spy on the activities of its citizens. It can only be hoped that the 21st Century will still have enough room from the individualist and the independently minded.
Seymour Krim (1987:133) described the world of New York after being discharged from a 'psych' hospital in the following terms:
"I returned downtown - to the very Village that I heard the psychiatrist place deep in Freudian Hell, with that pious overextension of terminology which reveals a limited private morality behind the use of so-called scientific language - and tried to tenderly pick up the threats of my former social life. I saw my closest and most brilliant friends did not really understand, or were afraid to understand, the contemporary insanity bit. Almost all of them had been soul-whirled by psychotherapy at some time, and each had the particularly contemporary fear of insanity, which has become the psychological H-bomb of city life; in theory they may have granted that insanity was no longer the uniform horror it seems to the inexperienced imagination - like the spook in the night - but centuries of inherited fear, plus the daily crises of 1950's living, made them emotionally cautious about seeing my experience as merely an extension of their own".
Laing, to the end, remained confident in the various aspects of the human condition.
"The human race seems able to order the universe in an indeterminable number of ways.
It has built and lived in many worlds.
We can sometimes just divine that all our worlds are variations on a theme, common to all, which, however, subsists and can be heard only in and through its variations, of which our contemporary world is one"
Laing, to the end, remained confident in humanity.
"The human race seems able to order the universe in an indeterminable number of ways.
It has built and lived in many worlds.
We can sometimes just divine that all our worlds are variations on a theme, common to all, which, however, subsists and can be heard only in and through its variations, of which our contemporary world is one"
R.D. Laing (1983:70)
Reference List
Barnes, M. (1973) ‘Flection/Reflection’, in Brown, P. (ed) Radical Psychology, N.Y., Tavistock Publications.
Barnes, M. (1975) Mary Barnes:Two Accounts of A Journey Through Madness, Harmondsworth, Penguin.
Basaglia, F. (1980) ‘Breaking the Circuit of Control,’ in Ingleby, P. (ed) Critical Psychiatry, Harmondsworth, Penguin.
Bateson, G. (1973) Steps To an Ecology of the Mind, N.Y., Palladin.
Bellow, S. (1971) Dangling Man, Harmondsworth, Penguin.
Binswanger, L. (1958) ‘The Case of Ellen West’ in May, R. (ed) Existence, N.Y., Simon and Schuster.
Breggin, P. (1994) Toxic Psychiatry, St. Martin’s Press.
Breggin, P. (1998) ‘Electric Shock: scientific, ethical, and political issues. International Journal of Risk & Safety in Medicine, 11, 5-40.
Breggin, P. (1995) Talking Back to Prozac, St. Martin’s Press.
Breggin, P. (2002) The Ritalin Fact Book, Cambridge, MA, Preseus Books.
Breggin, P & Breggin, G. (1998) The War Against Children of Color, Ian Allan.
Breggin, P. (2001) Dimensions of Empathic Therapy, Springer Publishing Company.
Brown, P. (1973) Radical Psychology, N.Y., Tavistock Publications.
Brown, P. (1974) Towards a Marxist Psychology, N.Y., Harper Colophon Books.
Chain, B.D. (1992) The Sayings of Sakyamuni Buddha, The Corporate Body of the Buddha Educational Foundation. Conrad, P.
Chain, B.D. (October, 1975) ‘The Discovery of Hyperkinesis’, Social Problems, 23:1, pp. 12-21.
Citizens Commission on Human Rights, (2005) website: http://204.13.211.146/index.cfm.
Cooper, D. (1967) Psychiatry and Anti-Psychiatry, N.Y., Palladin Books.
Cooper, D. (1971) ‘Beyond Words’, in Cooper, D. (Ed.) The Dialectics of Liberation, Harmondsworth, Pelican.
Cooper, D. (1972) ‘The Other Side of Therapy’, in Ruitenbeek, H. (ed) Going Crazy, N.Y., Bantam.
Cooper, D. (1974) The Death of the Family, Harmondsworth, Pelican.
Coper, D. (1980) The Language of Madness, Harmondsworth, Pelican.
de Zulueta, T. (1979) ‘No Patients - Just Consumers’, Guardian, 20 November.
Garton, S. (1988) Medicine and Madness, Kensington, N.S.W., New South Wales University Press.
Glenn, M . & Kunnes, R. (1973) Repression or Revolution, N.Y., Harper Colophon.
Goffman, E. (1975) Asylums, Harmondsworth, Pelican.
Gordon, J. (1972) ‘The Meta Journey of R.D. Laing.’, in Berke, J., Coles, R., Farber, L., Freidenberg, E. Lux, K., (ed) Laing and Anti-Psychiatry, Harmondsworth Penguin.
Gross, M. (1978) The Psychological Society, N.Y., Simon and Schuster.
Halleck, S. (1971) The Politics of Therapy, N.Y., Harper and Row.
Illich, I. (1977) Limits to Medicine, Harmondsworth, Penguin.
Inside Welfare ((March, (1979) An Annotated Bibliography For Marxist Welfare Workers, Sydney, Inside Welfare.
Jaffe, D. (1972) ‘A Halfway-Home Community.’, in The Radical Therapist Collective (ed) The Radical Therapist, Harmondsworth, Penguin.
Kerouac, J. (1972) On the Road, Harmondsworth, Penguin.
Kerouac, J. (1972) The Dharma Bums, G.B., Panther.
Kerouac, J. (1975) Maggie Cassidy, London, Quartet Books.
Kerouac, J. (1981) Big Sur, N.Y., McGraw-Hill.
Kerouac, J. (1981) The Subterraneans, N.Y. Grove.
Kerouac, J. (1985) Satori in Paris and Pic, N.Y., Grove Press.
Kerouac, J. (1988) Desolation Angels, Sydney, Grafton Books.
Kocan, P. (1980) The Treatment, Sydney, Angus & Robertson.
Koedt, A. (1970) ‘The Myth of Vaginal Orgasm.’, in Tanner, L. (ed) Voices From Women’s Liberation, N.J., New American Library.
Krim, S. (1987); 'The Insanity Bit' in Honan, H. (ed.) The Beats, Melbourne, J.M. Dent & Sons Ltd..
Lader, M. (1961) Psychiatry on Trial, Harmondsworth, Pelican.
Laing, R.D. (1961) The Divided Self, Harmondsworth, Penguin.
Laing, R.D. (1970) The Self and Others, N.Y., Pantheon.
Laing, R.D. (1971) ‘The Obvious.’, in Cooper, D. (ed) The Dialectics of Liberation, Harmondsworth, Penguin.
Laing, R.D. (1972) ‘Metanoia: Some Experiences At Kingsley Hall, London.’, in Ruitenbeek, H. et al (ed) Going Crazy, N.Y., Bantam Books.
Laing, R.D. (1977) The Facts of Life, Harmondsworth, Penguin.
Laing, R.D. (1978) The Politics of the Family and Other Essays, Harmondsworth, Penguin.
Laing, R.D. (1983) The Voice of Experience, Harmondsworth, Pelican.
Laing, R.D. (1984) The Politics of Experience and the Bird of Paradise, Harmondsworth, Penguin.
Laing, R.D. (1985) Wisdom, Madness and Folly: The Making of a Psychiatrist, London, Macmillan.
Laing, R.D. & Cooper, D. (1964) Reason and Violence, N.Y., Barnes and Noble.
Laing, R.D. & Esterson, A . (1971) Sanity, Madness and the Family, (2nd Edition), N.Y., Basic Books.
Langs, R. (1981) The Psychotherapeutic Conspiracy, the actual quote from Time Magazine, May, 1983.
Maslow, A. (1980) The Farther Reaches of Human Nature, Harmondsworth, Penguin.
May, P. (1968) Treatment of Schizophrenia, N.Y., Science House.
May, R. (1958)Existence, N.Y., Basic Books.
May, R. (1976) Power and Innocence, N.Y., Fontana.
Mead, G.H. (1934) Mind, Self and Society from the Standpoint of a Social Behaviourist, Chicago, University of Chicago Press.
Mebane- Francescato, D. & Jones, S. (1974) ‘Radical Psychiatry in Italy: Love is Not Enough.’, in the Radical Therapist Collective (ed) The Radical Therapist, Harmondsworth, Penguin.
Mezan, P. (1976) ‘R.D. Laing: Portrait of a Twentieth Century Skeptic.’, in Evans, R. (ed) R.D. Laing, The Man and His Ideas , N.Y., Tavistock
Publications.
Mills, C.W. (1973) The Sociological Imagination, Harmondsworth, Pelican.
Olson, D. (1972) ‘Marital and Family Therapy: A Critical Overview.’, in Gurman, A. & Rice, D. (ed) Couples in Conflict, N.Y., Behavioral Publications.
Orne, M. (1968) ‘On the Nature of Effective Hope.’, International J. of Psychiatry, Vol. 5, No. 5, pp.403-409.
Park, H. (ed) The Beats, London, J.M. Dent and Sons Ltd.
Radical Therapist Collective (1975) Therapy Means Change Not Adjustment, Harmondsworth, Pelican.
Sartre, J.P. (1953) Existential Psycho-analysis, Chicago, Gateway Books.
Sartre, J.P. (1965) Nausea, Harmondsworth, Penguin.
Sartre, J.P. (1977) Being and Nothingness, Secaucus, N.J., The Citadel Press.
Sedgwick, P. (1982) Psycho-Politics, London, Pluto Press.
Snyder, G. (1990) ‘All Through the Rains.’, in Hall, D. (ed) Contemporary American Poetry, 2nd Edition, Harmondsworth, Pelican.
Sorel, G. (1950) Reflections on Violence, London, Collier Books.
Spock, B. (1968) Baby and Child Care, N.Y., Pocket Books.
Steiner, C. (1975) Scripts People Live, N.Y., Bantam Books.
Stiegler, M. (1972) ‘Laing’s Model of Madness.’, in Freidenberg, G. (ed) Laing and Anti-Psychiatry, Harmondsworth, Penguin.
Suzuki, D. (1971) Living By Zen, London, Rider Pocket Edition.
Szasz, T. (1964) ‘The Moral Dilemma of Psychiatry.’, Am. J. Psychiat, 121, pp. 521-528.
Szasz, T. (1973a) Ideology and Insanity, Harmondsworth, Pelican.
Szasz, T. (1973b) ‘The Myth of Mental Illness.’, in Brown, P. (ed) Radical Psychology, N.Y., Tavistock Publications.
Szasz, T. (1984) The Therapeutic State, Buffalo, N.Y., Prometheus Books.
Szasz, T. (1988) The Theology of Medicine, N.J., Syracuse University Press.
Szasz, T. (1994) Cruel Compassion: Psychiatric Control of Society's Unwanted, N.Y. John Wiley & Sons.
Tennov, D. (1976) Psychotherapy: The Hazardous Cure, Garden City, N.Y., Anchor Books.
Throssell, H. ed. (1975) Social Work: Radical Essays, St. Lucia, University of Queensland Press.
Tsu Shu-Ying, (1992) ‘A Satori for Chao Chin Lin.’, in Sylvia, R. (ed) The Golden Dome of Eternity, to be published..
Zilbergeld, B. (1983) The Shrinking of America, N.Y., Little Brown.
Copyright © 2006
John Huddleston
Excluding photographs
(Anti-Psychiatry may not be reproduced, stored in a retrieval system, or transmitted in any form, by any means, including mechanical, electronic, photocopying or otherwise, without prior written permission of the writer.)